
Cardiovascular guidelines are considered the gold standard of evidence-based medicine. The recommendations of the European Society of Cardiology and the European Atherosclerosis Society for lowering LDL cholesterol are clear, differentiated by risk profiles, and supported by numerous randomized controlled studies. Nevertheless, in everyday care, a clear discrepancy has been evident for years between these recommendations and their actual implementation. This is particularly evident in the example of statin therapy.
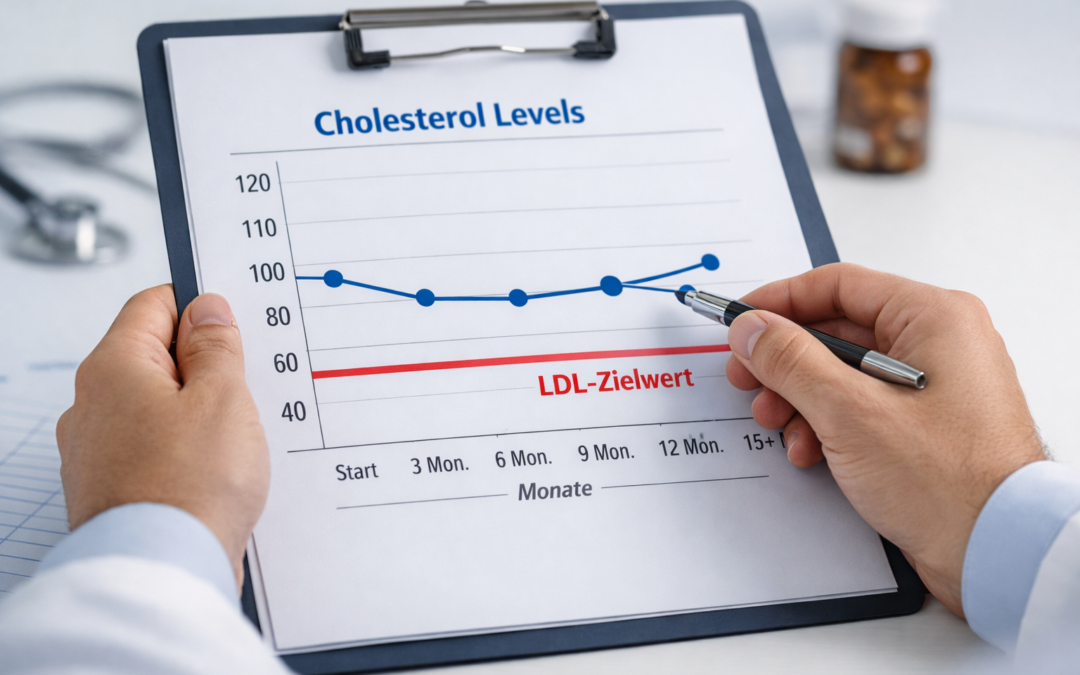
Real-world data from European cohorts show that only about 30 to 40 percent of patients with high or very high risk achieve the recommended LDL target values. This gap cannot be explained by a lack of pharmacological efficacy. In randomized studies, statins reliably lower LDL cholesterol and significantly reduce cardiovascular events. The causes lie rather in the practical use of the therapy.
A key factor is adherence. Around half of patients discontinue an initiated statin therapy within one to two years. The reasons are diverse and range from subjectively perceived side effects to a lack of understanding of the disease and insufficient medical counseling. Controlled studies also show that a considerable proportion of reported statin-associated symptoms can be explained by nocebo effects (negative effects without a causal relationship between intervention and effect). However, this discrepancy between perceived and actual drug tolerability is rarely addressed systematically in everyday practice.
In addition to therapy discontinuation, underdosing and a lack of therapy escalation also play a decisive role. Despite insufficient LDL reduction, many patients remain on low statin doses for years without receiving combination therapies or intensification in accordance with guidelines. Lack of time, therapeutic hesitation, concern about side effects, or a lack of structured follow-up monitoring contribute to this. Lack of time, therapeutic hesitation, concern about side effects, or a lack of structured follow-up monitoring contribute to this.
For health services research, this gap between efficacy under study conditions and effectiveness in everyday practice is highly relevant. While randomized controlled trials primarily examine the biological efficacy of a drug, real-world data reflect actual care. For health policy decisions, health technology assessments, and benefit evaluations within the framework of AMNOG procedures, these data are becoming increasingly important, as they capture effects on hard endpoints, healthcare costs, and long-term outcomes.
At the same time, this reveals a starting point for improvements. Greater use of real-world data can help identify gaps in care early and address them in a targeted manner. The topic of patient engagement is also coming into focus. Informed, engaged patients show higher adherence and a better understanding of the benefits and risks of long-term prevention. Informed, engaged patients show higher adherence and a better understanding of the benefits and risks of long-term prevention.
Digital solutions can support this by facilitating continuous support of therapy, promoting adherence, and improving communication between the practice and the patient. Anyone aiming to effectively shape cardiovascular prevention must take this reality into account and, in addition to pharmacological evidence, also focus on implementation, communication, and long-term support. Digital support solutions such as the mediteo app can contribute here by making therapy processes more transparent and accompanying patients in everyday life without replacing the physician’s decision-making process.
Sources
- Wood FA, Howard JP, Finegold JA et al.: Effects of statin therapy on muscle symptoms: an individual patient data meta-analysis of large-scale randomised, double-blind trials.
The Lancet. 2022;400:832–845.
Effect of statin therapy on muscle symptoms: an individual participant data meta-analysis of large-scale, randomised, double-blind trials - Mann DM, Woodward M, Muntner P et al.: Achievement of guideline-recommended LDL cholesterol levels among high-risk patients in contemporary European cohorts. European Heart Journal.
- Chowdhury R, Khan H, Heydon E et al.: Adherence to cardiovascular therapy: a meta-analysis of prevalence and clinical consequences.
BMJ. 2013;346:f116; Adherence to cardiovascular therapy: a meta-analysis of prevalence and clinical consequences | European Heart Journal | Oxford Academic - Mach F, Baigent C, Catapano AL et al.: 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. European Heart Journal. 2020;41(1):111–188; https://academic.oup.com/eurheartj/article/41/1/111/5556353
Back to Blog.